Acute Renal Failure (ARF) — now more commonly referred to as Acute Kidney Failure — is a sudden loss of the kidneys’ ability to filter waste, electrolytes, and fluid from the blood. This rapid decline can develop within hours or days, causing dangerous levels of waste products to accumulate in the body and disturbing fluid balance.
It most often occurs in people who are critically ill, hospitalized, or undergoing major surgery.
Diagnosis or treatment is initiated when a patient presents with:
Sudden drop in urine output
Swelling (edema) in legs, ankles, or around eyes
Fatigue and confusion
Nausea, vomiting
Shortness of breath
Chest pain or pressure
Irregular heartbeat
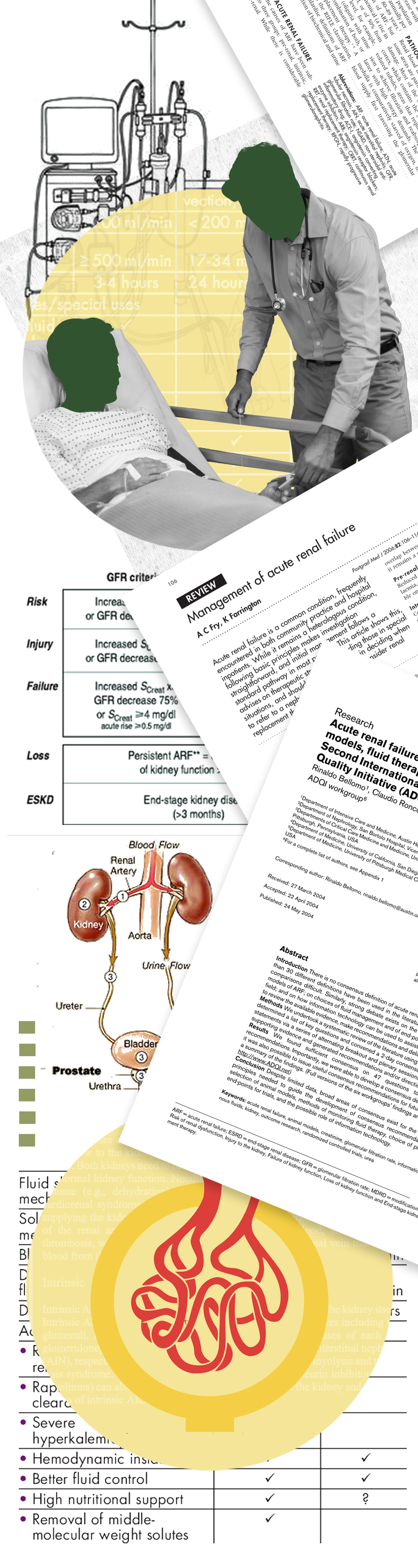
Acute renal failure may result from:
Reduced blood flow to kidneys (e.g., dehydration, heart failure)
Direct kidney damage (e.g., infections, toxins, drugs)
Blockage of urinary tract (e.g., enlarged prostate, stones)
If ARF is suspected, initial steps involve:
Blood tests (Creatinine, BUN, electrolytes)
Urinalysis
Imaging (Ultrasound, CT)
Stopping nephrotoxic drugs (e.g., NSAIDs, contrast dyes)
For treatment, vascular access (like a central line) may be required if dialysis is initiated. No special prep is needed for medical management unless specific procedures are performed.
There’s no single "procedure" for ARF — treatment depends on the cause and severity:
Hospitalization is often required
IV fluids to restore hydration if dehydration is the cause
Diuretics may be used if kidneys are overloaded but not producing urine
Temporary dialysis may be needed to manage fluid, toxins, and electrolytes
Medications are adjusted or stopped if they’re causing kidney damage
Ongoing monitoring includes:
Urine output
Electrolyte levels
Daily weight and fluid balance
Blood pressure
Recovery may take days to weeks:
Some patients recover full kidney function, especially with early intervention
Others may progress to chronic kidney disease or require long-term dialysis
Frequent follow-ups are needed post-discharge
Expect:
Restricted fluid intake
Low protein or low potassium diets
Multiple lab tests and imaging during recovery
Complications of ARF can be life-threatening and include:
Fluid overload
Elevated potassium levels (hyperkalemia)
Acidosis (low blood pH)
Uremia (toxic waste buildup)
Seizures or coma
Permanent kidney damage or death in severe cases
Early detection and proper supportive care significantly reduce these risks.
Prognosis depends on:
Underlying cause
Severity of illness
Age and comorbid conditions
Outcomes:
Full recovery is possible in many cases
Some patients may develop chronic kidney impairment
Mortality risk is high in critically ill or elderly patients
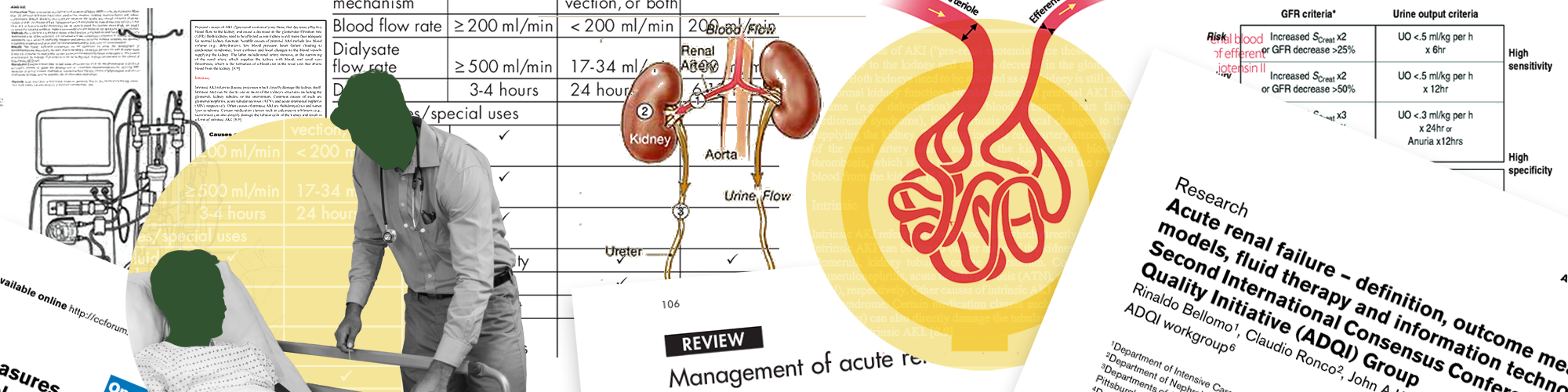
Lab markers like serum creatinine, BUN, and glomerular filtration rate (GFR) are tracked to gauge progress.
For patients recovering from ARF:
Dietary restrictions (e.g., salt, potassium, fluid)
Avoid nephrotoxic medications
Regular kidney function tests
Hydration management
Lifestyle guidance focuses on:
Controlling blood pressure
Managing diabetes (if present)
Preventing infections
Nephrologist: Oversees diagnosis and treatment
Hospitalist or ICU Team: Provides supportive care
Dietitian: Assists with renal-friendly diet planning
Nurse: Monitors fluid status, medications, labs
Clinical Trials may explore:
New biomarkers for earlier detection
Protective medications to reduce kidney injury
Techniques for renal recovery post-critical illness