Polycystic (polly-SIS-tick) kidney disease (PKD) is a genetic disease. It is caused by a change (mutation) in your genes. There are different genetic mutations that can cause PKD.
PKD causes clusters of cysts to develop within the kidneys causing the kidneys to enlarge and hypofunction. This is a benign, inherited condition that has fluid-filled round cysts. Moreover, these cysts can grow large but often vary in size. Their size can greatly affect renal function and may involve the liver and other organs. Thousands of cysts can grow in your kidneys and cause a kidney to weigh up to 30 pounds! This disease has severe complications if not attended to on time. Some complications are associated with chronic kidney disease (CKD), which can lead to kidney failure, or end-stage renal disease (ESRD).
There are two types of PKD: autosomal dominant PKD and autosomal recessive PKD.
| Autosomal dominant PKD (ADPKD) | Autosomal recessive PKD (ARPKD) | |
|---|---|---|
| What happens in this type of PKD? | ADPKD causes cysts to grow in your kidneys. About half of people with ADPKD will have kidney failure by age 70. Over time, ADPKD can also affect other organs, especially the liver. | ARPKD causes cysts to grow in your kidneys. It can be severe and deadly for newborn babies. More than half of all children who survive will have kidney failure by the time they are 15 to 20 years old. ARPKD can also affect other organs, especially the liver. |
| When do symptoms start? | Symptoms often start when you are between 30 and 50 years old, which is why it is also called "adult PKD". | Symptoms start in babies, sometimes even before they are born, which is why it is also called "infantile PKD". |
Autosomal dominant PKD (ADPKD) is the most common type of PKD and one of the most common genetic kidney diseases. About 9 out of every 10 people with PKD have ADPKD. ADPKD causes cysts to grow in your kidneys and can also affect other organs, especially the liver.
ADPKD is caused by a change (mutation) in a specific gene. Most people with ADPKD have a change in one of these genes: PKD1 or PKD2. ADPKD runs in families and does not skip a generation. This means that if you have ADPKD, it is very likely one of your parents also had or has a change to the PKD1 or PKD2 gene, even if they have not been diagnosed.
Unlike some genetic diseases, ADPKD does not skip a generation meaning it often affects many people in one family. Approximately 10 percent of the people diagnosed with ADPKD have no family history of the disease, with the disease developing as a spontaneous (new) mutation. Once a person has ADPKD, even through a spontaneous mutation, they have a 50 percent chance of passing it on to each of their children.
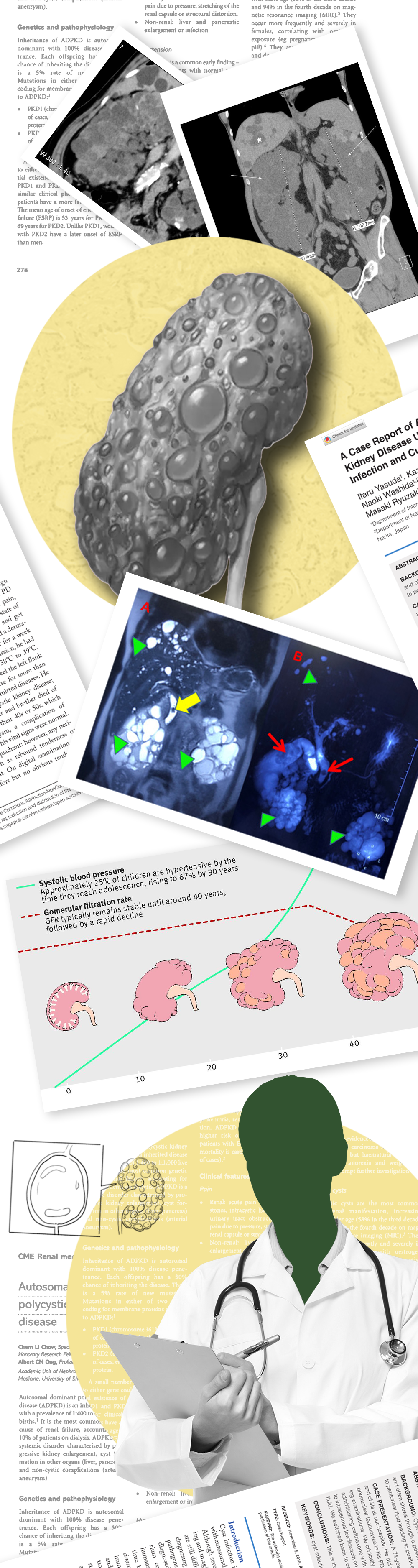
Symptoms usually start when you are between 30 and 50 years old. Symptoms include:
Pain in your back and sides
Headaches
Blood in your urine (pee)
High blood pressure
UTIs (urinary tract infections)
Kidney stones
A feeling of fullness in the abdomen. Enlarged kidneys cause an increase in the size of the abdomen
Currently, there are three main tests that are used to screen for ADPKD:
Ultrasound
Computed tomography (CT)
Magnetic resonance imaging (MRI)
Ultrasound is the most common and least costly screening method for PKD. There are accepted standards for ultrasound testing to determine if you have PKD. These standards include the number of cysts visible, age, and family history.
CT and MRI scans are considered to be more sensitive than ultrasound. CT scans, however, involve radiation or may also require iodinated contrast dye which, can be toxic to the kidneys. CT scans or MRIs may be used to look at complications like bleeding into a cyst or a suspected kidney stone. They may also be used detect small cysts as needed.
DNA testing is available for PKD. There are two types of DNA tests: Gene linkage testing and direct mutation analysis/DNA sequencing. Gene linkage can determine if you have PKD with a 99 percent probability in those with family history. Linkage testing is not a direct analysis of the DNA sequence of the PKD1 and PKD2 genes. Instead, it relies on the identification of certain “markers” in the DNA of several members of a family in which PKD has been diagnosed. For linkage analysis, blood samples must be obtained from the person being tested as well as several (typically three or more) family members including those affected and unaffected by PKD. A detailed family history is also required. The results are typically reported to all family members that provided blood samples for the analysis.
In contrast, direct DNA sequencing requires only a single sample from you (the person being tested). This method is a direct analysis of the DNA sequences of the PKD1 and PKD2 genes. It is private, and the results are only reported to you and your doctor.
Using very specialized scientific equipment, each of the nearly 17,000 “bases” of DNA are analyzed and the entire sequence is thus determined.
This method is capable of identifying those changes in the sequence that cause PKD. It may be your only option if family members are unavailable or unwilling to participate in a linkage study. Each of these methods could be costly and should not be done without consideration of the pros and cons.
Health, life and disability insurance coverage vary between countries and may influence your decision to have genetic testing. In the United States, the Affordable Care Act has guaranteed health insurance for all regardless of any preexisting conditions. This does not guarantee life or disability coverage.
A diagnosis of PKD should be carefully considered and discussed with your doctor.
When your kidneys are not working as well as they should, it can cause other health problems such as:
More than eighty percent of patients with PKD develop liver cysts during their lifetime. Liver cysts can occur in those under the age of 30, but are usually small and detectable only by MRI scanning. The liver can remain normal in size with a few cysts or can become enlarged. Even with increased liver size from PKD, the amount of functional liver tissue remains more than adequate. This means it is highly unlikely that patients with severe polycystic liver disease (PLD) would develop liver failure.
Although not common, severe PLD can present with symptoms due to a “mass effect” (i.e. abdominal fullness, pain, early satiety (feeling full), ankle swelling and fluid accumulation within the abdomen). In the severe and symptomatic cases, cyst decompression may be needed. When a few very large cysts are present, additional surgical intervention may be recommended to take care of these cysts. Partial liver resection may be considered in selected cases. This should only be performed at specialized centers with experienced surgeons.
Liver cysts occur more often in women than men. Women develop liver cysts at a younger age and have more and larger cysts than men. Women with previous pregnancies have more numerous and larger liver cysts than women without any pregnancies. This observation suggests that female hormones may influence the development of liver cysts. Because estrogen may be a factor in liver cyst growth, the benefits of estrogen replacement therapy (ERT) and the risk of PLD must be carefully weighed. A Nurses’ Health study has disproved any benefit of estrogen to prevent cardiovascular disease, however, estrogen replacement therapy is protective against osteoporosis and decreases vasomotor instability – a cause of hot flashes in postmenopausal women. Thus, the risk of estrogen for aggravating PLD against its potential benefits on post-menopausal symptoms and osteoporosis needs to be weighed. Work with all of your doctors (nephrologist, Ob/Gyn, and general practitioner) to determine what would be the best course for you.
Women with PKD who use estrogen after menopause should have a baseline ultrasound of their liver before they start ERT and every two years thereafter. This will help your doctor evaluate if liver cysts are increasing in number and/or size. It is unclear at this time if it is better to take ERT in pill form or by skin patch. Theoretically, the patch would be a better choice since oral therapy provides high concentrations of estrogen directly to the liver. Finally, there is no data looking at the effect of low-dose oral contraceptives on women with ADPKD. If you have significant PLD, you should discuss the use of these with your doctor.
One complication of PLD is liver cyst infection. Symptoms range from fever to pain in the upper right side of the abdomen. These symptoms need to be reported to your doctor as soon as possible. Treatments of an infected liver cyst usually require antibiotic therapy and occasionally needle drainage.
Mitral valve prolapse (MVP) is a condition where the valve separating the top and the bottom of the left side of the heart does not close properly. Sometimes this causes blood to leak back to the top part of the heart. This is called regurgitation and can be heard during an examination of the heart as a heart murmur. Symptoms that can be associated with MVP are palpitations, a feeling that the heart is running away or that there are extra beats in the heart and chest pain that is not associated with exercise or exertion. MVP occurs with increased frequency in patients with PKD as compared to the general population but rarely causes any significant clinical problems.
MVP is usually confirmed with an ultrasound of the heart valves called an echocardiogram. If MVP is present and causes palpitations that are bothersome, they can be treated with medications. Restricting the use of caffeine, alcohol, and
cigarettes may be enough to decrease or stop the palpitations in many cases.
Rarely, an infection of a heart valve can occur as a complication of MVP. Although not a common occurrence, it can lead to destruction of the heart valve. Therefore, if you have MVP and a heart murmur, inform all doctors who care for you.
An aneurysm is an outpouching in a blood vessel, which can leak or rupture.
Intracranial (brain) aneurysms occur in the blood vessels of the brain. Symptoms can include sudden severe headache, pain in moving your neck, nausea/vomiting, difficulties with speech or movement and/or loss of consciousness. A ruptured aneurysm can be fatal. If you know you have an aneurysm (or have a family history of aneurysms) and you are experiencing any of these symptoms, you should call emergency services immediately.
Recent studies done in the United States have shown that PKD patients have about a 5 – 10 percent risk of developing intracranial aneurysms. This is about five times the risk of the general population. They also seem to cluster in certain families – that is, if a member of your family has an aneurysm or has ruptured an aneurysm, you may be at a higher risk of having an aneurysm yourself.
Because the risk for aneurysm is small, not everyone with PKD needs to be tested. However, people who have PKD and a family history of aneurysm should be tested, along with those whose job or hobbies would put them or others at risk if they lost consciousness (such as those who fly airplanes or drive buses). It is important to inform your doctor if you have a family history of intracranial aneurysms and/or if you have a high-risk occupation or hobby.
Aneurysms in other vessels such as the aorta have also been reported.
Magnetic resonance angiography (MRA) is the preferred test to screen for an aneurysm.
When an aneurysm is detected on an MRA, an arteriogram is usually performed. This test is more invasive and is done by putting dye directly into the blood vessels which will more clearly show if there is an aneurysm and how large it is.
If an aneurysm is found, surgical repair or a therapeutic coil (a device placed in the aneurysm by a neuroradiologist) may be recommended. If and when surgery is performed depends on the size and location of the aneurysm. Often an aneurysm can be repaired surgically before it leaks or ruptures. If you have had one aneurysm, you may develop others over time and need periodic follow-up. Recent studies suggest that patients with a positive family history of ICA should be screened with MRA every 5-10 years.
Both inguinal and umbilical hernias are more common in those with PKD. Inguinal hernias are outpouchings in the area of the groin. Umbilical hernias are outpouchings at or near the navel. These should be surgically repaired if they are large or are causing problems, just as they would be in someone who does not have PKD.
Diverticula are outpouchings on the large intestine (colon). It appears that patients with PKD who are on dialysis or have had a transplant have diverticula more often and also have more complications from diverticula, including infection, than patients with other kidney diseases.
Diverticulitis can occur when diverticuli rupture or become infected, requiring treatment with antibiotics. This is a rare occurrence.
A recent study found that ADPKD patients face elevated risk of diabetes after a kidney transplant.
The Canadian Journal of Diabetes reports a detailed analysis of 12 studies, which comprised 1,379 patients with ADPKD of a total of 9,849 patients who had undergone kidney transplants and found that individuals with ADPKD who undergo a kidney transplant have a higher association of new-onset diabetes than non-ADPKD kidney transplant patients. These findings may impact disease management of ADPKD patients before transplant and follow up after transplant.
In a comment from SAC member Ronald Perrone, M.D. “In light of this study, the advice I have for patients is that maintaining a healthy diet and healthy weight both before and after transplant are key to avoiding an increased risk of type 2 diabetes”.
Kidney failure or ESRD–more than half of people with ADPKD have kidney failure by age 70 and it happens more in Black people compared to white people
UTIs (urinary tract infections)
Kidney stones
A problem during pregnancy called preeclampsia (a type of high blood pressure)
High blood pressure
Chronic pain
There is no cure for ADPKD. Your doctor can recommend strategies to manage some of the symptoms and health problems caused by ADPKD. There is also an option that can slow the progression of ADPKD to kidney failure.
After you find out that you have ADPKD, it is important to work with your doctor to understand your risk for progressing to kidney failure and learn about what you can do to manage it. Following your management plan and making healthy life changes may be able to help you keep your kidneys working longer and slow progression to kidney failure.
Take these steps to slow the damage to your kidneys:
Work with your doctor to prevent or manage diabetes and high blood pressure.
Keep a healthy weight.
Take all of your prescription medicines as your doctor tells you.
Follow a kidney-friendly eating plan. A dietitian can help you make a plan that works for you.
Be active for at least 30 minutes most days of the week.
Drink less or quit alcohol. The healthy guidelines for drinking alcohol are:
Quit smoking or using tobacco.
Some people with ADPKD are at a higher risk for progressing to kidney failure than others. If your kidneys fail, you will need to start dialysis or have a kidney transplant to live.
Treating people with autosomal dominant polycystic kidney disease often aims to improve renal function. Other factors that determine the treatment option are the severity of the disease, the patient's age, condition, and tolerance to the treatment.
The early treatment of autosomal dominant polycystic kidney disease requires managing the associated conditions apart from the disease itself. Medicines that help manage the disease include:
Blood pressure control: Medicines such as angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs) are prescribed to manage high blood pressure.
Blood sugar control: Medicines that help control high blood sugar in people with diabetic nephropathies, such as metformin, improve insulin sensitivity and lower glucose production in the liver. Glucagon-like peptide 1 (GLP-1) receptor agonists reduce blood sugar levels by slowing digestion and stimulating insulin secretion in response to rising glucose levels. SGLT2 inhibitors limit glucose from returning to the bloodstream, leading to increased glucose excretion in the urine.
Kidney cyst growth: Tolvaptan therapy is often recommended for adults who are at risk of rapidly progressive ADPKD. Tolvaptan helps slow the rate of cyst growth and improves renal function.
Pain: Pain with polycystic kidney disease may be excruciating, and need over-the-counter medications to alleviate it. Sometimes, sclerosing treatments are advised for people with constant and unbearable pain. Alternatively, removing the cysts may also be an option for some.
Bladder or Renal Infections: Immediate treatment of infections is necessary for a patient with polycystic kidney disease. This is because untreated cases may damage the kidney entirely and may lead to sepsis. Antibiotics help treat these infections. Sometimes, longer therapy may be required for complex infections.
If the kidney disease progresses to kidney failure (end-stage kidney disease), the treatment is focused on either replacing the kidneys or using a dialyser to remove toxins from the body. In addition, the treatment aims at making the patient more comfortable. Some options include:
This treatment is done to remove waste products and extra fluid from the blood. The two main types of dialysis are:
Hemodialysis - It is more commonly done and requires regular visits to the dialysis centre about three times a week. Alternatively, a trained caregiver can do dialysis at home for a session of 3 to 5 hours a week.
Peritoneal dialysis - This procedure can be done either at home or at a dialysis centre.
In some cases, the best option is a kidney transplant. If a kidney transplant is chosen, the patient's eligibility as a recipient is tested.
Autosomal recessive polycystic kidney disease (ARPKD) is a rare genetic disorder that affects 1 in 20,000 children. A fetus or baby with ARPKD has fluid-filled kidney cysts that may make the kidneys too big, or enlarged. ARPKD can cause a child to have poor kidney function, even in the womb. ARPKD is sometimes called “infantile PKD” because health care providers can diagnose it so early in life.
Poor kidney function can cause breathing problems that can threaten the life of a fetus or baby. A baby with ARPKD who survives birth and the first few weeks of life has a good chance of surviving into adulthood. However, children or young adults with ARPKD will likely need medical treatment their whole life.
ARPKD is caused by a change in a specific gene called PKHD1 that is passed down from both parents to their child. Both parents need to be carriers of the changed PKHD1 gene for their child to be born with ARPKD. If only one parent carries the mutated gene, the child will not get the disorder, although the child may get the gene mutation. The child is a “carrier” of the disorder and can pass the gene mutation to the next generation.
How quickly ARPKD progresses to kidney failure is different for each child. The sooner a fetus is diagnosed in the womb, the better the child’s outlook. Getting good prenatal care is important for increasing a child’s survival rate. Working with a health care team as soon as possible can help parents manage their child’s PKD.
Symptoms can start before a baby is born, at birth or in childhood.
Ultrasound images the mother has while pregnant show that the unborn baby's kidneys are larger than they should be
Not enough amniotic fluid around the baby–amniotic fluid is the liquid that surrounds and protects the baby in the mother's womb. In the middle to later months of pregnancy, the baby's kidneys should make amniotic fluid. Some babies with ARPKD have damaged kidneys even before birth, and their kidneys cannot make enough amniotic fluid.
Lung immaturity and functioning issues
Throwing up breast milk or formula after feeding
Problems with how the baby's face, arms and legs grow
Enlarged kidneys due to cysts
Breathing problems due to lack of space because of enlarged kidneys and decreased urine production. Ventilation is frequently required to sustain life.
Excessive urine production
Hypertension
Congenital hepatic fibrosis
Enlarged spleen with low red blood cell, white blood cell and platelet counts
Some children with ARPKD may not have any symptoms. Children with more severe ARPKD may have:
High blood pressure
UTIs (urinary tract infections)
Pain in their back or side
Varicose veins (large veins that you can see through their skin, often in their legs)
Lower than average height and weight
Typically in ARPKD, the kidneys appear to be larger than normal. In some babies, prenatal ultrasound can detect the enlarged kidneys as early as 18 weeks after conception. Some families may also hear their doctor say the kidneys look “echogenic” (more white) during an ultrasound, which can be an indicator of kidney problems such as ARPKD.
Prenatal genetic testing is possible using samples from either chorionic villus sampling or amniocentesis. These genetic tests can either involve a direct search of the gene for mutations or an indirect association using linkage analysis. For linkage analysis, DNA samples are required from the fetus, a previously affected child, and the parents.
Another option for pre-natal diagnosis in affected families is a recently developed procedure called pre-implantation genetic diagnosis, or PGD. This is an early form of genetic diagnosis that involves the detection of specific genetic abnormalities in single cells taken from fertilized human embryos. The PGD procedure involves in vitro fertilization whereby eggs harvested from a mother are fertilized in a laboratory with the father’s sperm. Then, the fertilized embryos are tested for ARPKD by removing one or two cells for genetic analysis. Embryos that are diagnosed as free of the disorder are then placed in the uterus with the intent to initiate a pregnancy.
ARPKD may cause any of these other health problems:
Kidney failure before adulthood
UTIs (urinary tract infections)
ARPKD affects both kidneys and the liver. Affected children may have significant kidney involvement at the time of birth. In-utero, urine production is a critical factor in maintaining normal amniotic fluid levels. When amniotic fluid levels are very low, lung development can be impaired. In some newborns with low levels of amniotic fluid, impaired lung development can result in serious breathing difficulties that require ventilation upon birth and sometimes can cause death.
Children with ARPKD often produce very large volumes of urine and must urinate much more frequently than children with normal kidneys. Given the kidney abnormality, urine production in ARPKD children does not slow down at night or even when liquid intake is limited.
High blood pressure is very common in children with ARPKD, and current information indicates that untreated high blood pressure can lead to kidney failure more quickly than if the blood pressure is kept within the normal range with medications. Most children with ARPKD have high blood pressure.8 High blood pressure increases a child’s chances of heart disease and stroke.
Children with ARPKD also have the liver abnormality called congenital hepatic fibrosis (CHF) that may lead eventually to enlargement of the liver and spleen. In the liver, the abnormality can impede the return of blood from the intestine to the liver. This condition, called portal hypertension, can lead to distention and increased pressure in the veins around the esophagus, the stomach, and the intestine. This can rupture, leading to possibly life-threatening gastro-intestinal bleeding. In addition, portal hypertension can cause spleen enlargement and hypersplenism resulting in low red blood cell, white blood cell and platelet counts.
There is no cure for ARPKD. Doctors can recommend strategies to help manage the symptoms and health problems that ARPKD causes. Management strategies may include.
Enlarged kidney: Kidney enlargement cannot be prevented or reversed. One or both kidneys may need to be removed if their size makes breathing impossible. Children who don’t have working kidneys will need dialysis or a kidney transplant.
Growth failure: A health care provider may treat growth failure with nutritional therapy NIH external link. In severe cases of growth failure, a health care provider and a child’s parents may consider treatment with human growth hormone. Human growth hormone is a prescribed, man-made hormone that can help children grow.
Breathing problems: Health care providers treat infants with breathing problems with artificial ventilation, which allows them to breathe with the help of a machine.
Kidney failure: Peritoneal dialysis is the preferred method of treating children with kidney failure, although health care providers also use hemodialysis. Kidney transplants may be a limited option for infants because of their size.
Liver problems: If serious liver disease develops, some children may need to have a combined liver and kidney transplant.
High blood pressure: A health care provider can help control blood pressure with medicines. Treating high blood pressure can help delay kidney failure.
Yes, the genes for ADPKD are dominant, which means that inheriting only one mutated copy of the PKD1 or PKD2 gene from an affected parent is sufficient to cause the disease. There is no carrier state with a dominant disease, and it does not skip a generation. This means that the disease will eventually manifest as you get older and that all generations have the potential to be affected. If you have a mutation, at some point in your life at least some of the symptoms of the disease will probably occur, although they could be very mild. When an at-risk individual does not have a mutation for ADPKD, he/she is not affected and the disease cannot be passed to the next generation.
This does not mean that everyone who gets the ADPKD gene will have the same signs or symptoms or the same course of the disease. There is a wide spectrum of severity within ADPKD. At one end are children who are diagnosed before birth or in the first year of life with cysts or big kidneys, at the other end are people who have few symptoms, even when they are much older. It is important to note that some individuals (especially those with a PKD2 or non-inactivating PKD1 mutation) are more likely to live a normal life span and die of other causes before there is a need for dialysis or transplantation. A majority of patients with ADPKD will fall in the middle and at some point in their life will have some signs or symptoms associated with ADPKD.
Yes, all affected ADPKD patients with the same mutation in a family will have the same type of ADPKD. However, their signs, symptoms and course of the disease are often different. The most dramatic example of this occurs in families with children who are diagnosed before birth or in the first year of life. These children have symptoms long before their parents. Sometimes the parent may not even be aware they have ADPKD until after their child is diagnosed. Significant kidney disease variability within ADPKD families suggest other genetic and environmental factors can modify the severity of this disease.
Just as in adults, children who have ADPKD are more likely to have mitral valve prolapse (MVP) and hernias than children who do not have ADPKD. Approximately 12 percent of all ADPKD children will have MVP, but unlike adults, it is unusual for them to have any symptoms. If your child has a hernia, they should be treated as they would in any other child. Children rarely have any of the other manifestations of ADPKD.
Acquired cystic kidney disease (ACKD) is not a type of PKD. Like PKD, people with ACKD have fluid-filled cysts growing inside their kidneys. However, people are not born with ACKD. ACKD is caused by chronic kidney disease (CKD) or kidney failure. Unlike PKD, people with ACKD do not have cysts in other organs.
ACKD is more common in people who have had kidney disease for a long time. ACKD happens most often in people who are on dialysis, but dialysis does not cause cysts.