Immunosuppressive drugs are medications that reduce or suppress the strength of the body’s immune response. They are commonly used in organ transplantation to prevent rejection, and in autoimmune diseases to control an overactive immune system attacking the body's own tissues. These medications help restore immune balance but require close monitoring due to potential side effects.
Immunosuppressive therapy is prescribed to:
Prevent organ transplant rejection (kidney, liver, heart, lung, etc.)
Treat autoimmune disorders such as:
Systemic lupus erythematosus (SLE)
Rheumatoid arthritis
Psoriasis
Inflammatory bowel disease (Crohn’s/Ulcerative Colitis)
Multiple sclerosis
Manage glomerulonephritis and other immune-mediated kidney diseases
Control cytokine storms in severe infections (e.g., COVID-19 related hyperinflammation)
These medications are essential when the body’s immune system becomes harmful to its own cells or newly transplanted organs.
Pre-treatment Evaluation Includes:
Blood tests: CBC, liver/kidney function, infection markers
Screening for infections: Hepatitis, TB, HIV, etc.
Vaccination status: Updated before starting long-term immunosuppressants
Baseline imaging or organ function tests (especially in transplant patients)
Access:
Most immunosuppressive drugs are administered:
Orally (pills/capsules)
Intravenously (IV infusions)
Subcutaneously (e.g., biologics)
The route depends on the type of drug, condition, and urgency
This isn’t a single procedure but a long-term medication protocol, often involving a combination of drugs. Key classes include:
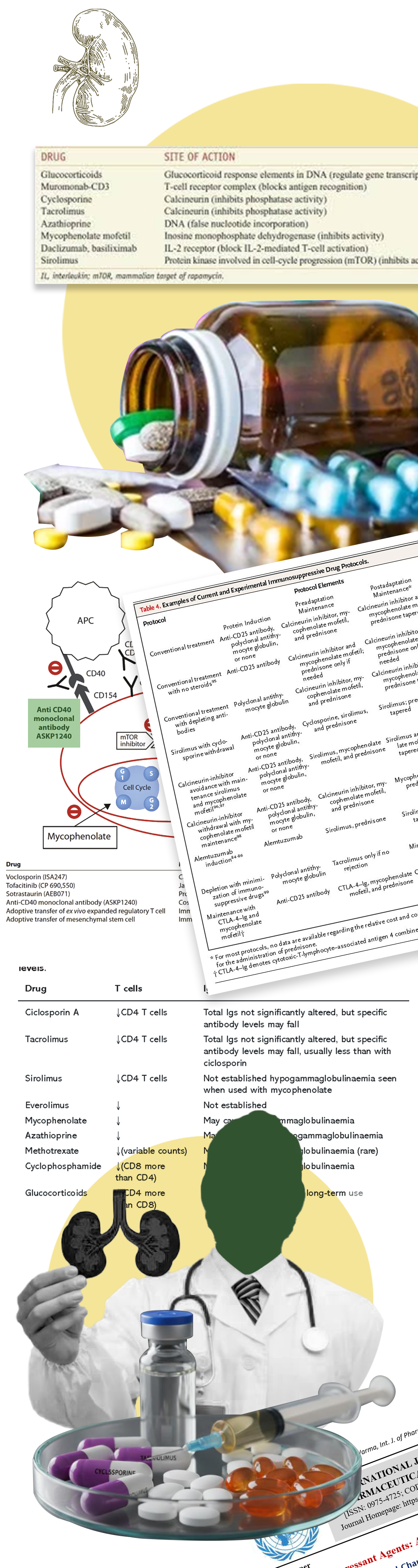
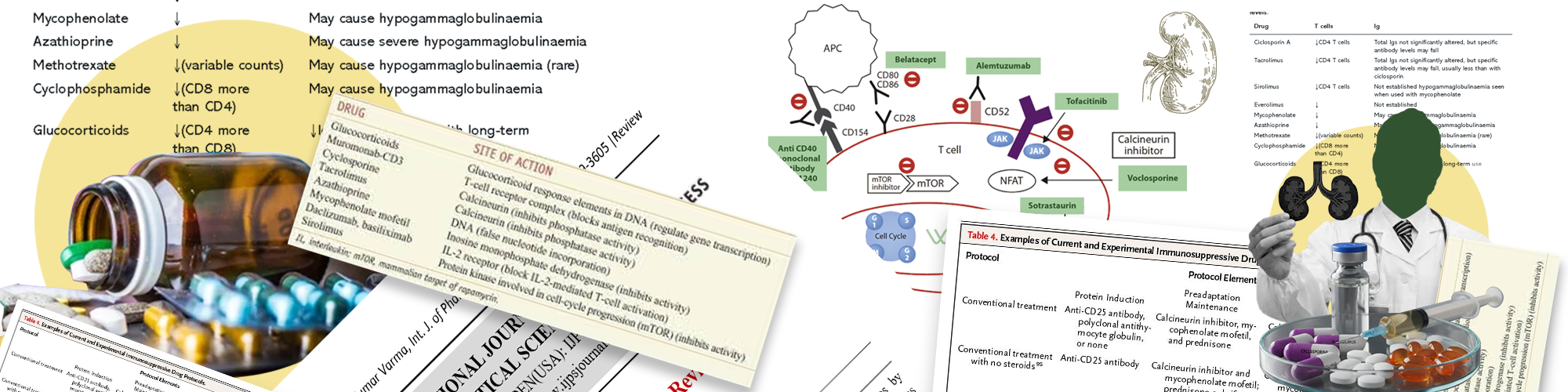
Corticosteroids (e.g., Prednisone) – Reduce inflammation quickly.
Calcineurin Inhibitors (e.g., Tacrolimus, Cyclosporine) – Prevent T-cell activation.
Antimetabolites (e.g., Azathioprine, Mycophenolate mofetil) – Block immune cell growth.
Biologics & Monoclonal Antibodies (e.g., Rituximab, Adalimumab) – Target specific immune pathways.
mTOR Inhibitors (e.g., Sirolimus) – Block cell proliferation.
JAK Inhibitors (e.g., Tofacitinib) – Used in autoimmune diseases.
Drugs are often layered to balance immune suppression and side effect risks.
Long-term, often lifelong treatment (especially post-transplant)
Frequent lab monitoring (e.g., drug levels, organ function, white cell counts)
Regular follow-ups with nephrologist, rheumatologist, or transplant team
Adjustments in dose based on clinical response and lab results
Strict adherence is critical to prevent flare-ups or organ rejection
Lifestyle adjustments may be required to reduce infection risk (e.g., avoiding crowded places, raw foods, live vaccines).
Common risks include:
Infections (due to weakened immune defenses)
Increased cancer risk, especially skin cancers and lymphomas
Liver or kidney toxicity (depending on drug type)
High blood pressure or diabetes
Bone thinning (osteoporosis) with long-term steroid use
GI upset, weight gain, acne, mood changes
Each drug class carries its own specific side effects; hence close monitoring is crucial.
When used appropriately, immunosuppressive drugs can:
Dramatically improve quality of life in autoimmune conditions
Significantly increase organ transplant survival
Reduce frequency and severity of disease flares
Stabilize or improve organ function, particularly kidneys and joints
Success is measured through:
Disease remission or symptom control
Stable graft function in transplants
Biomarker and imaging improvements
Avoid infections: Maintain hygiene, wear masks, avoid exposure.
Vaccinations: Only inactivated vaccines allowed; coordinate with care team.
Dietary restrictions: Some meds require avoiding grapefruit or alcohol.
Routine bloodwork: Every 2–6 weeks based on disease and medication.
Mental health support may be needed due to chronic treatment nature.
Adherence to medication and lifestyle guidance is essential for long-term success.
Primary Physician/Rheumatologist/Nephrologist: Manages overall care and medication
Transplant Physician (if applicable): Manages rejection surveillance and drug titration
Pharmacist: Ensures correct dosing and checks drug interactions
Nursing Team: Educates patients, monitors side effects
Lab & Imaging Technicians: Provide necessary data for decision-making
Ongoing research & trials:
Safer drug combinations with fewer side effects
Precision medicine approaches using genetic markers
Next-gen biologics and immune modulators