Arteriovenous (AV) fistula creation is a surgical procedure where an artery is directly connected to a vein, typically in the arm. This connection increases blood flow through the vein, making it stronger and wider for long-term hemodialysis access. It is considered the gold standard for dialysis access due to its durability and lower risk of complications.
AV fistulas are created in patients with advanced chronic kidney disease or end-stage renal disease (ESRD) who are expected to need regular hemodialysis. It is preferred over catheters and grafts because it:
Offers better blood flow for effective dialysis.
Reduces the risk of infection and clotting.
Lasts longer than other access types.
Before the procedure:
Vein mapping (ultrasound) is done to assess vein suitability.
Anticoagulants or blood-thinning medications may be adjusted.
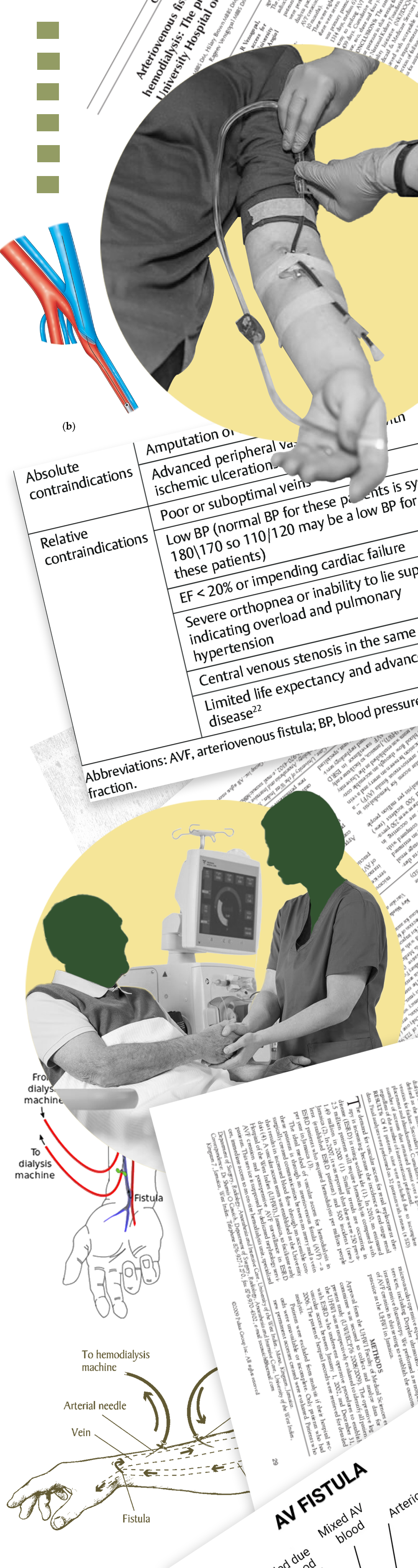
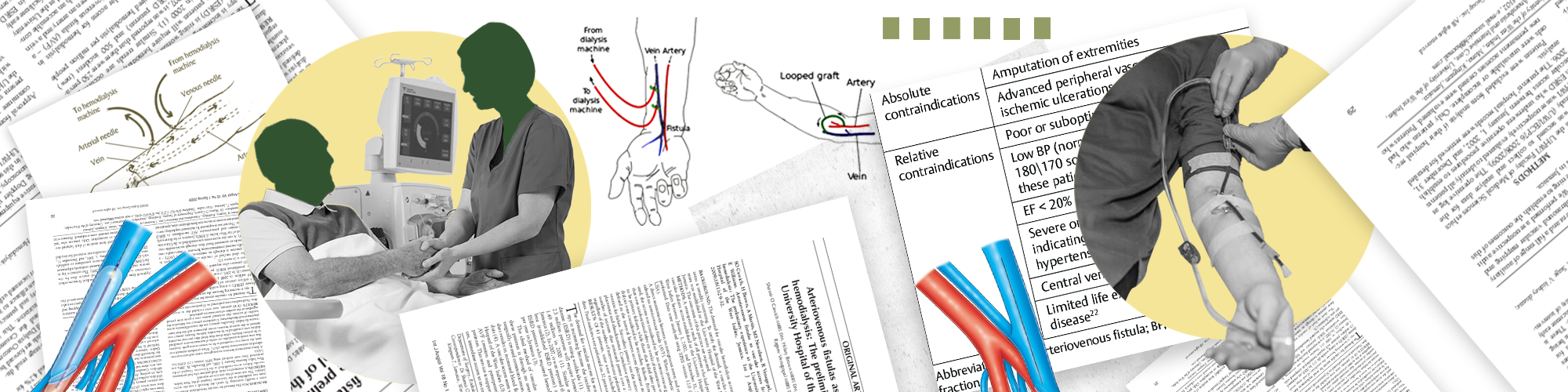
The most common sites are the radiocephalic (wrist) and brachiocephalic (elbow) regions.
Types of AV fistulas:
Radiocephalic fistula – between the radial artery and cephalic vein (wrist).
Brachiocephalic fistula – between the brachial artery and cephalic vein (elbow).
Brachiobasilic fistula – deeper vein brought to the surface in two stages.
Typically done under local anesthesia in an outpatient surgical setting.
A small incision is made in the arm.
The surgeon connects an artery and a nearby vein.
The skin is closed with sutures, and a sterile dressing is applied.
The entire process may take 1–2 hours, and patients can usually return home the same day.
Maturation period: 6–12 weeks for the fistula to become usable (the vein becomes thickened and strong).
Routine check-ups to assess blood flow and detect narrowing or failure.
You may feel a “thrill” or vibration at the site, indicating proper blood flow.
Once matured, the fistula is used 3 times a week during dialysis, with two needles inserted at each session.
While AV fistulas are generally safe, possible complications include:
Non-maturation (fistula doesn’t develop well).
Steal syndrome (reduced blood flow to the hand).
Infection or clot formation.
Aneurysm formation due to repeated needle insertion.
Early detection and intervention reduce long-term risks.
AV fistulas are associated with:
Lower hospitalization rates.
Longer functional life span compared to catheters or grafts.
Improved dialysis efficiency (better blood flow = better toxin removal).
Better patient outcomes, including survival and quality of life.
Protect the arm: No blood draws, BP checks, or tight clothing.
Avoid sleeping on the access arm.
Hand and arm exercises may be recommended post-surgery to improve fistula maturation.
Maintain hygiene and monitor for redness, swelling, or loss of thrill.
Nephrologist: Identifies need and coordinates access planning.
Vascular Surgeon: Performs the procedure.
Dialysis Nurse/Technician: Monitors access site during dialysis.
Radiologist: Conducts imaging if problems arise.
Current research and clinical trials focus on early maturation, novel surgical techniques, and biomaterial-based fistulas.