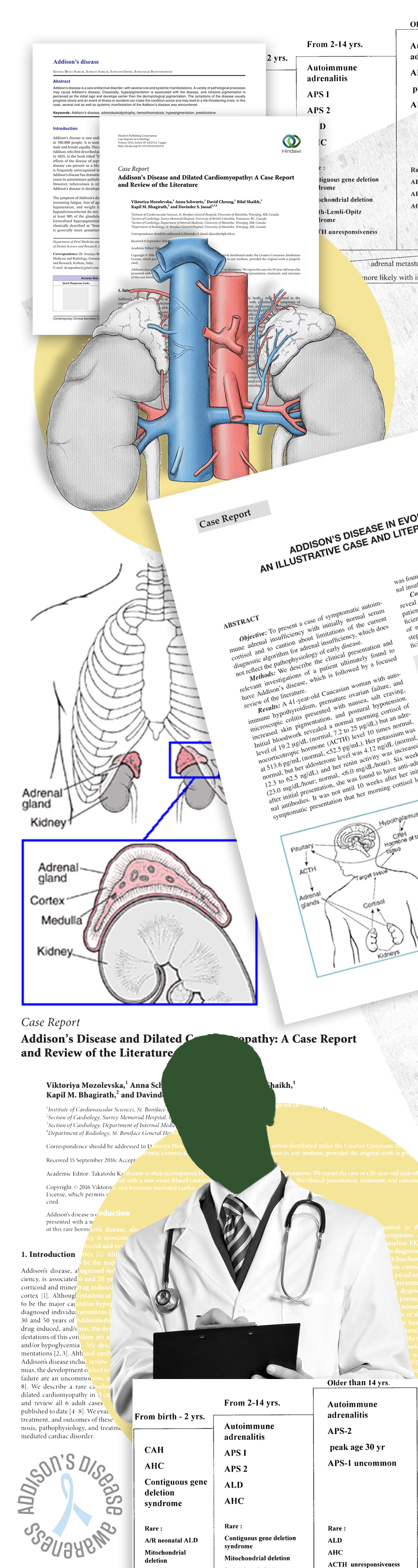
Addison’s disease (also known as primary adrenal insufficiency) is a rare disorder that occurs when the adrenal glands fail to produce enough cortisol and aldosterone — two essential hormones that help the body respond to stress, regulate blood pressure, and maintain salt-water balance.
The condition can develop slowly over time or present suddenly as an Addisonian crisis, a life-threatening medical emergency.
Addison’s disease is diagnosed and treated when individuals present with symptoms such as:
Extreme fatigue
Unexplained weight loss
Low blood pressure, especially when standing
Skin darkening (hyperpigmentation)
Salt craving
Nausea, vomiting, or abdominal pain
Muscle or joint pain
Irritability, depression
The condition may be triggered by:
Autoimmune destruction of adrenal glands (most common cause)
Infections like tuberculosis or fungal diseases
Cancer metastasis
Bleeding into the adrenal glands
Prompt diagnosis is essential to prevent an Addisonian crisis — marked by severe hypotension, shock, and electrolyte imbalances.
Tests and evaluations for diagnosing Addison’s disease include:
ACTH stimulation test (to evaluate cortisol response)
Blood tests (to check sodium, potassium, cortisol, ACTH levels)
Imaging (CT or MRI scans to evaluate adrenal glands)
No special access (e.g., surgical access) is needed for diagnosis, but IV access may be required for urgent treatment during a crisis
Treatment primarily involves hormone replacement therapy, which is lifelong:
Oral corticosteroids:
Hydrocortisone, prednisone, or cortisone acetate to replace cortisol
Fludrocortisone acetate to replace aldosterone if needed
In times of stress (illness, surgery, etc.), the dosage may need adjustment to prevent crisis
In case of an Addisonian crisis:
Immediate IV hydrocortisone, saline, and dextrose are administered
Hospitalization is often required
Patients are educated to:
Carry an emergency steroid injection kit
Wear a medical alert bracelet
Double steroid dose during illness or injury
With proper treatment:
Most people with Addison’s disease lead normal, active lives
Hormone replacement becomes a daily lifelong routine
Regular follow-up with endocrinologists is essential
However, untreated or mismanaged Addison’s can result in:
Frequent fatigue
Hormonal imbalance symptoms
Life-threatening Addisonian crises
If not treated properly, Addison’s disease can lead to:
Addisonian crisis: sudden, severe symptoms requiring emergency care
Low blood pressure and shock
Severe dehydration
Electrolyte imbalances (especially hyperkalemia and hyponatremia)
Over-replacement of steroids can cause:
Weight gain
Osteoporosis
Diabetes or elevated blood sugar
Cushingoid symptoms if long-term doses are excessive
With consistent treatment and monitoring:
Most individuals manage symptoms effectively
Quality of life is preserved
Routine hormone level monitoring ensures proper dosing
Outcomes are best when:
Emergency care is available for Addisonian crisis
Patients adhere to stress dosing protocols
Regular endocrinologist follow-ups are maintained
Lifestyle modifications include:
Regular medication timing (same time daily)
Increased salt intake (especially in hot climates or with aldosterone deficiency)
Stress management and avoiding overexertion
Keeping emergency hydrocortisone injection and alert ID handy
Patients should:
Be vigilant during infection, surgery, or trauma
Avoid skipping doses or self-adjusting medication
Endocrinologist: Manages long-term hormone therapy
Primary care physician: Monitors overall health, electrolytes
Emergency care team: Manages Addisonian crisis
Dietitian: Guides on sodium intake, nutrition
Clinical trials are investigating:
Long-acting hydrocortisone formulations
Alternative cortisol replacements with fewer side effects
Gene therapies and autoimmune modulation