Sustained Low Efficiency Dialysis (SLED) is a hybrid renal replacement therapy combining features of intermittent hemodialysis (IHD) and continuous renal replacement therapy (CRRT). It runs over an extended period (typically 6–12 hours) using lower blood and dialysate flow rates—providing gradual, gentle solute and fluid removal suited for hemodynamically unstable or critically ill patients.
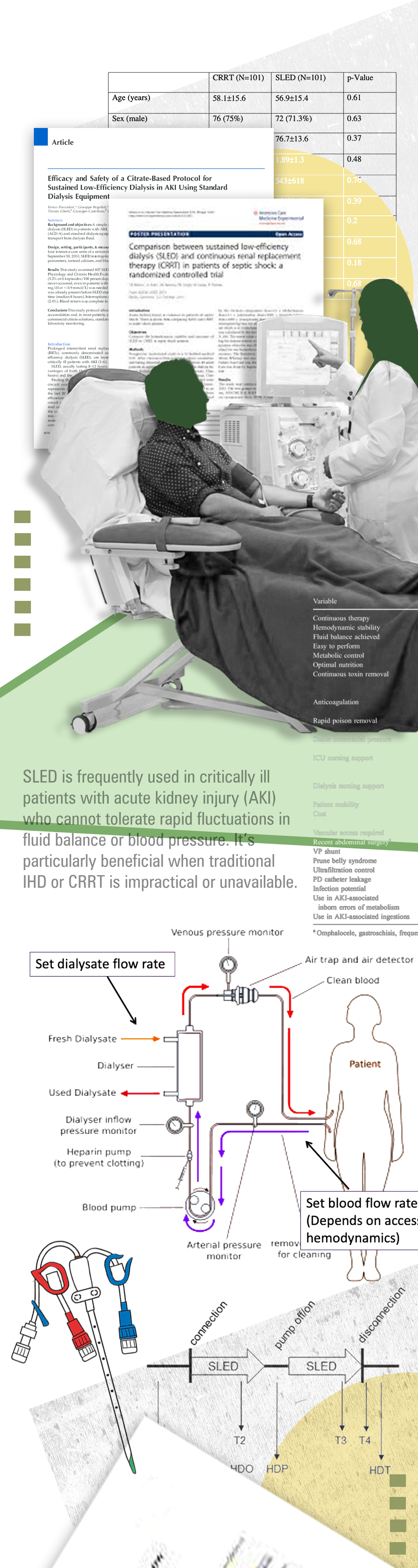
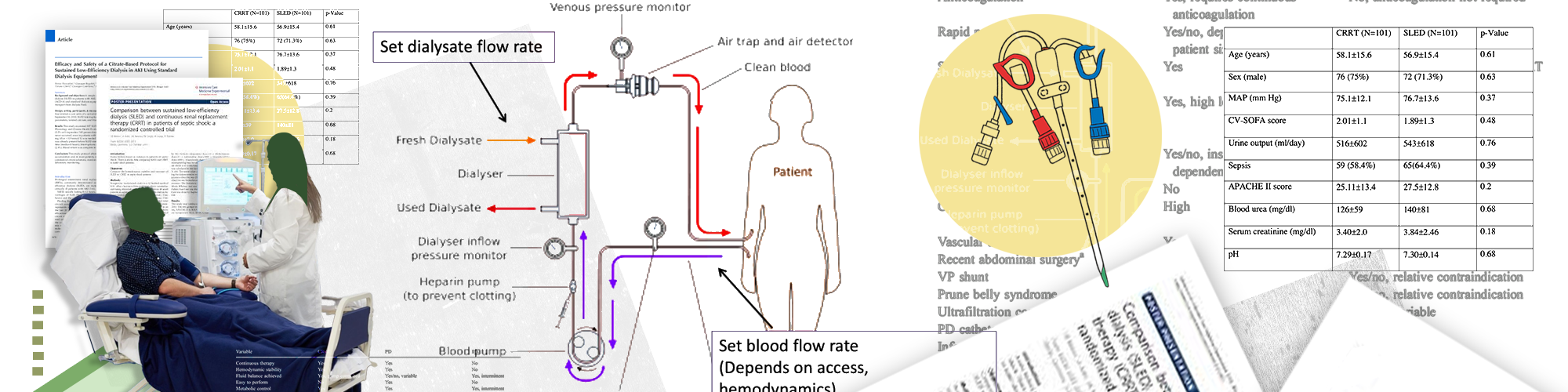
SLED is frequently used in critically ill patients with acute kidney injury (AKI) who cannot tolerate rapid fluctuations in fluid balance or blood pressure. It’s particularly beneficial when traditional IHD or CRRT is impractical or unavailable.
SLED is typically delivered via standard HD machinery using blood flow rates around 150–250 mL/min and dialysate flow around 300–350 mL/min. A session lasts 6–12 hours, allowing cleaner, gentler toxin and fluid removal. It can also be adapted as SLED-F (adding hemofiltration) or C-SLED (continuous version for extended duration in unstable patients).
Compared to CRRT, SLED offers similar clearance of solutes and cardiovascular stability, while being more cost-effective and easier to manage using standard dialysis equipment. It's often chosen if conventional IHD fails or CRRT resources are limited.
Reduces hypotensive episodes by gradual fluid removal.
Comparable small-molecule clearance to CRRT and IHD.
Sessions can be arranged around patient care or ICU workflows.
Often performed without systemic heparin, using saline flushes instead
Up to 40 50% lower ICU cost compared to CRRT in some studies
While gentler than IHD or CRRT, SLED still poses risks:
Dialyzer clotting, especially without anticoagulation.
Electrolyte imbalances (e.g. hypophosphatemia) require close monitoring
Lower efficiency in rapid waste removal; not ideal in situations needing immediate clearance.
Limited access: Requires trained staff and extended machine occupancy.
Continuous clinical monitoring is essential—track vital signs, hemodynamic stability, circuit integrity, anticoagulation status, and electrolytes (especially phosphorus and potassium). Remote alerts or telemetry are often employed in ICU settings to quickly flag machine alarms or clotting events
Clinical outcomes (30-day mortality, renal recovery) are frequently comparable between SLED and CRRT.
In studies of patients with AKI, SLED demonstrated a lower incidence of transfusion need, fewer days on mechanical ventilation, and shorter ICU stay.
Nutritional support may be needed during extended SLED regimens, especially in cancer or critically ill patients